

Info Overview
Overview
CheckIron is a loss making charity, we deliberately make, nor, ask for, money. Our purpose is to promote the fact that Prevention of Hemochromatosis is possible through Genetics alone and we can provide support for all Hemochromatosis sufferers including sufferers who are carriers. The reason for being loss making is to gain the trust of our users who we believe need to be shown our sole purpose is to help the Hemochromatosis community and their genetically related relatives as much as we can. We rely on the scientific papers written on Hemochromatosis and the Genetic data of our users to teach our software what the genes that cause inflammation really are. We find discussions with doctors and even on the FB Hemochromatosis(HH) groups has too much dogma and incorrect assumptions at its basis and we often see people saying things that do not fit with the scientific research and our data. This is very disappointing as there seems to be huge disconnects in particular between the scientists and the doctors.
There are many information sources for Hemochromatosis, but many are inconsistent with each other and some are even inconsistent within themselves between documents from the same source. Things like treatment using diet, how many genes are involved in Hemochromatosis, whether carriers can overload iron and even the definition of Hemochromatosis itself. This is not only confusing, it's also disappointing that such a mess is made of it. And it's even worse than that because it's clear there is also a major difference between many doctors and the scientists measuring the effects of Hemochromatosis and investigating the Iron Metabolism. Furthermore, at CheckIron, we've obtained additional data no-one has had before which strongly indicates what genes are implicated in Hemochromatosis to the extent that we now believe prevention of Iron Overload is possible by just looking at genes and then predicting when excessive levels would normally occur and taking proactive preventative action. This is something no-one has suggested before simply because the data we've used has never been collected before.
Prevention
There are some excellent information resources on Hereditory Hemochromatosis(HH). Each country has a charitable or semi-charitable organisation which provides very useful help and advice for people diagnosed and suffering from Hereditory Hemochromatosis. The problem we have concerning these information resources is they provide no positive help for prevention of Iron Overload and little to no information on how genetics can be used to determine someone's risks. The reason for these ommisions is historical as 10-15 years ago many of the scientific experts were saying that prevention by genetic screening for Hemochromatosis was not possible or sensible. For example, at that stage it was thought that a small percentage of people with the high risk gene mutations would actually be symptomatic for HH - figures like 10% penetration were often given for even the worst Homozygous C282Y mutations were given. Since then much further scientific work has been done and real measurements have now been published. The published figure for Homozygous C282Y biological penetration is 77% and the reason why this is not 100% is simply that some people have other mutations which slows the overload process so much that many die before they become overloaded. There was also an issue which is not admitted in that DNA analysis was very expensive at that stage and certainly medical organisations did not want to feel the pressure of being asked to screen for Hemochromatosis.
HH Carriers
There are also often ommissions about HH carriers. It was always known that a very low percentage of carriers suffered from Iron Overload, in fact its now known that only between 1-2% of carriers do suffer from iron overload. The medical profession have picked up on this number and simplified it to the extent that some often say there are "no risks for carriers". In fact statistically, they will be right for 98% of the time they say it and for these people its correct to not worry about it ever again. However, for the 1-2% left this is very incorrect advice. Further more this 1-2% of people is rather a large number of people, because between 8% and 23% of the whole population are indeed carriers. The table below shows the actual numbers for the US
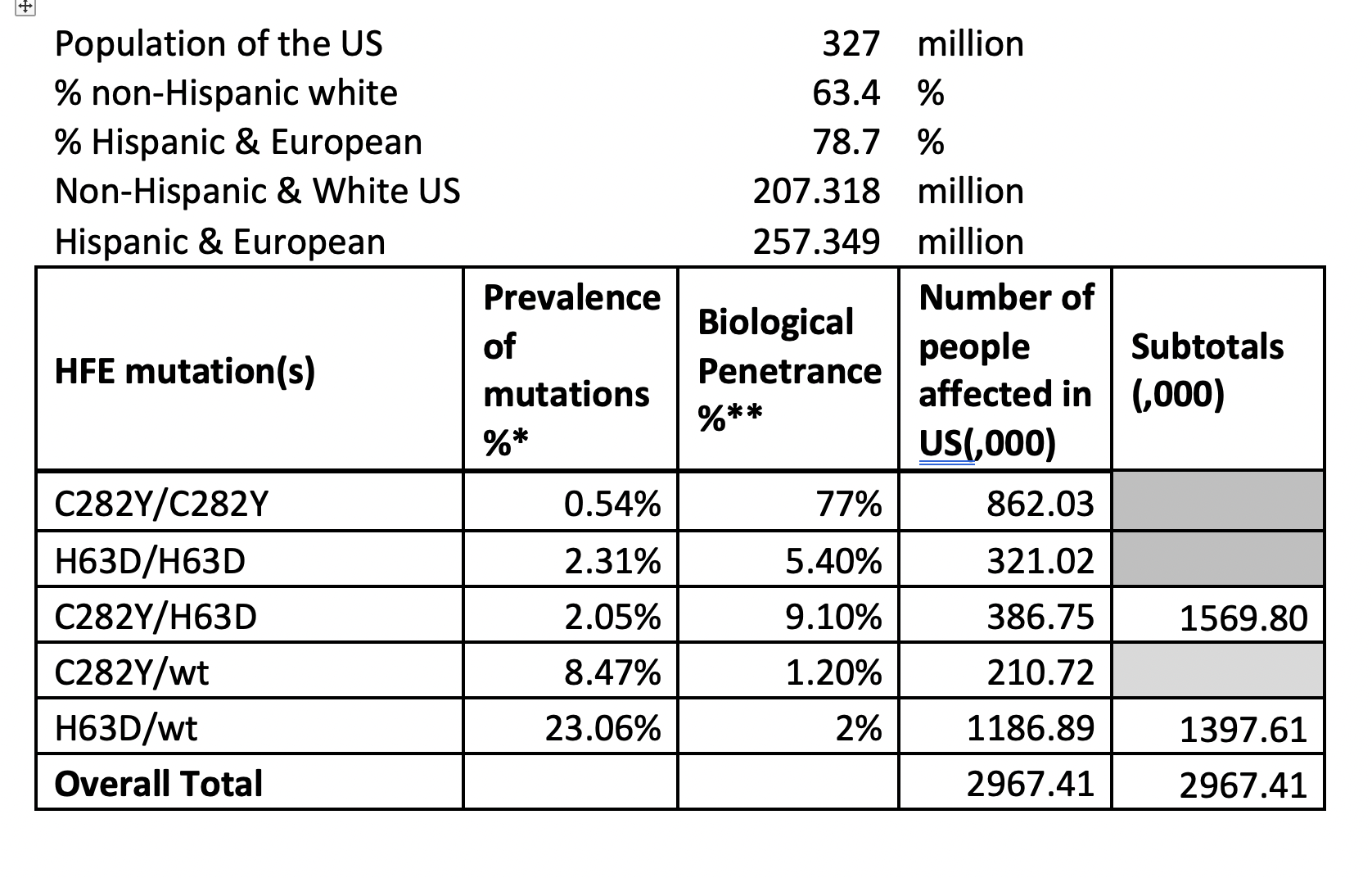
* https://jamanetwork.com/journals/jama/fullarticle/193800
** https://hal.archives-ouvertes.fr/hal-00535020**
You can see from the above table that there are more H63D carriers (H63D/wt) suffering from Iron Overload than there are Homozygous C282Y people who, we are often told, are the most common suffers. Very few in the Hemochromatosis community state or even know this statistic fact correctly at all.
So even though there is a lot of useful information in the other online HH resources there is also some important ommissions and even incorrect statements because they are presenting information 10-15 years out of date. So here we present the latest scientific informations.

Prevention using Genetic prediction of Age at Symptoms
In the overview section we've introduced the concept that a DNA test can help determine the risks for the user. We also explained that historically this approach was not believed possible and even today most people including most medical experts will say that Prevention using a DNA test is not possible.
Current guidelines (the best of such Guidelines is BHS Diagnosis and therapy of genetic haemochromatosis (review and 2017 update)) still only suggest DNA tests for close relatives of homozygous C282Y sufferers and for others it suggests blood tests for ferritin and transferrin saturation are the main ways to determine risks with later possible support of a DNA test only if iron levels are determined to be raised. It's, of course this way round, because historically DNA tests have been expensive and it is believed to be a cost saver to do the cheaper blood test first. This cost saving is debatable because by waiting for the blood iron levels to be raised enough to indicate Hemochromatosis the patient is exposing him/herself to iron levels which can cause signficant organ damage. This is the basis of the problem we have with this approach - we believe that we can show that a commercial DNA test alone can predict when someone will get symptoms.
Now let's look at the types of Genetic Testing. There are 2 main ways of a patient getting a Hemochromatosis Genetic test. The first is from
your doctor who will do a genetic blood test -often this test is limited to looking just a the mutations of the HFE gene but in some cases it
can be extended to look at many more mutations such as listed in this picture. 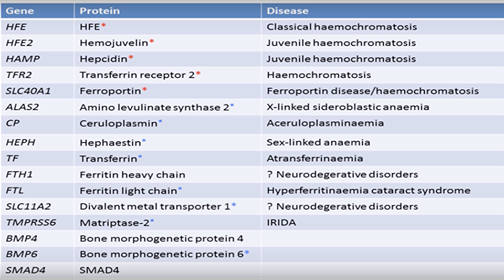 .
.
This list
of 16 genes is more useful but is still missing the important BMP2 gene mutations. This youtube video describes the work being done here and says
this test costs the NHS £500. (see this video for the details of the specialised 16 gene NHS test)
Meanwhie the second way is for you to do a more extensive tests using one of the commercially available tests from the Family Tree type DNA tests (eg Ancestry, 23andMe, MyHeritage, FamilyTreeDNA etc). These tests look at hundreds of thousands of mutations and the result is that because of the extra data a more extensive analysis can be performed. Indeed, it's the use of these tests which has enabled us to spot patterns missed by the very limited testing performed by the medical profession. The cost of these tests can be as low as US$99 and even lower at times of special offers. Often people say these commericial tests are not medical grade and indeed they are not medical grade but it is better to consider accuracy. The accuracy of these medical tests is no different to the accuracy of these commercial tests, but they do not have the label "medical grade". In my experience though my doctor had no problem with my AncestryDNA result - he totally accepted it.
At the time of writing (Feb 2024) we've had nearly 2000 uploads in CheckIron V3.1 but only have had 550 of those that told us their age when they got symptoms. We had hoped for more, but this has been enough to give us some confidence that there is a pattern between certain mutations and the age at symptoms. In fact we discovered that the age of symptoms for Hemochromatosis is dependent on 4 major factors (this is a simplified view):
- The HFE gene mutation - C282Y or H63D in every combination (double, single or combined)
- The transferrin mutations - we found that BMP2 and Pro570Ser in particular mutations speed up loading and the G277S mutation slows loading.
- The risks of other inflammatory diseases. The immune system uses iron to control inflammation - in fact if someone is suffering inflammation the immune system will try to shut down iron absorption and convert free iron to ferritin - this is called Anaemia of Inflammation. The problem is if someone has HFE mutations the production of Hecidin to reduce iron absorption will be either reduced or zero dependent which mutations the person has. The result is iron continues to flow into the body and ferritin levels rise even more. The result is the rate of iron coming into the body increases. At a certain point the amount of iron in the body is so much that conversion to ferritin becomes harder and iron itself causes futher inflammation resulting in out of control iron levels and iron overload
- There are 4 other different genes which can cause Hemochromatosis. These are all thought to be rare but our analysis of 2,000 sample shows HH Type 3 (TFR2 gene) mutations are not rare and indeed do affect iron overload. In fact it seems quite common for people to have both HFE mutations and TFR2 mutations at the same time (more of this later)
These 4 factors are highly significant whereas we believe many others are just using the HFE mutations are the single indicator of Hemochromatosis and as a results carriers and even combined mutations are being ignored as being significant. We believe all the combinations are signficant in the presence of the transferrin mutations which increased transferrin.
So that was the simplified view. Currently the calculations are raw estimates but over time and with increasing input from users uploading their data we hope to make these estimates more accurate. We do accept that external factors like, diet, and blood loss through menstruation or blood donation also have a non genetic input to the age at symptoms.
Age at Symptoms
Hemochromatosis causes iron to build up in the body over time. So it's ususally at an older age people suffer most. But why is it that for the same genetic mutation there is a wide range ages people begin to suffer (we call this the age at symptoms).
| Homozygous C282Y | Compound C282Y/H63D | Homozygous H63D | H63D Carrier | C282Y Carrier | No HFE Mutations | |
|---|---|---|---|---|---|---|
| Penetrance Chart | 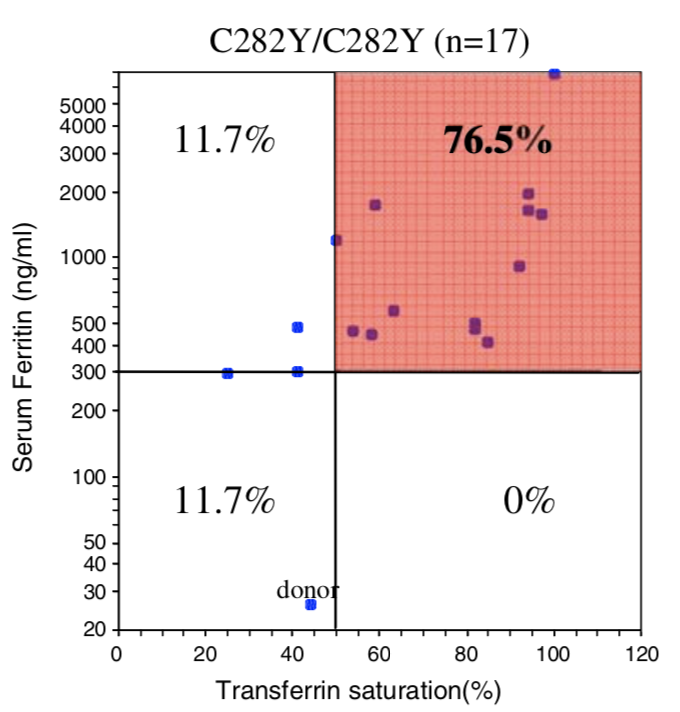 |
 | 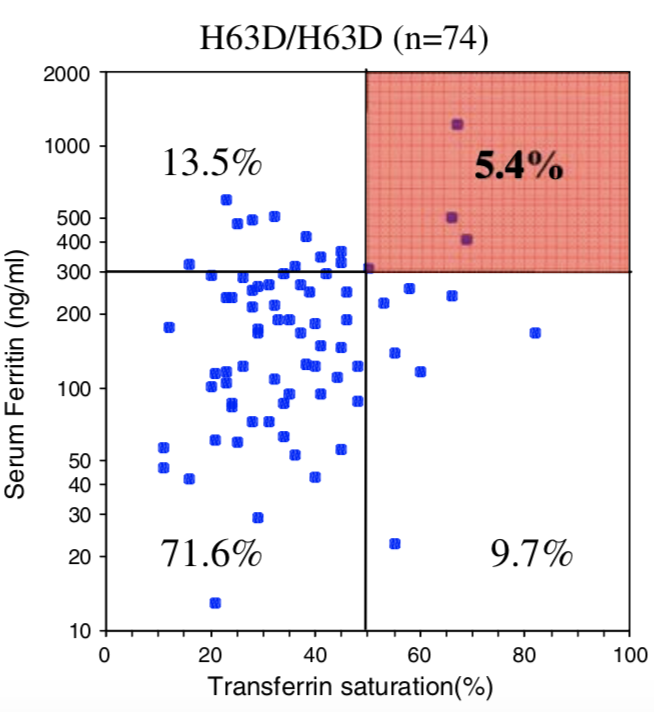 |
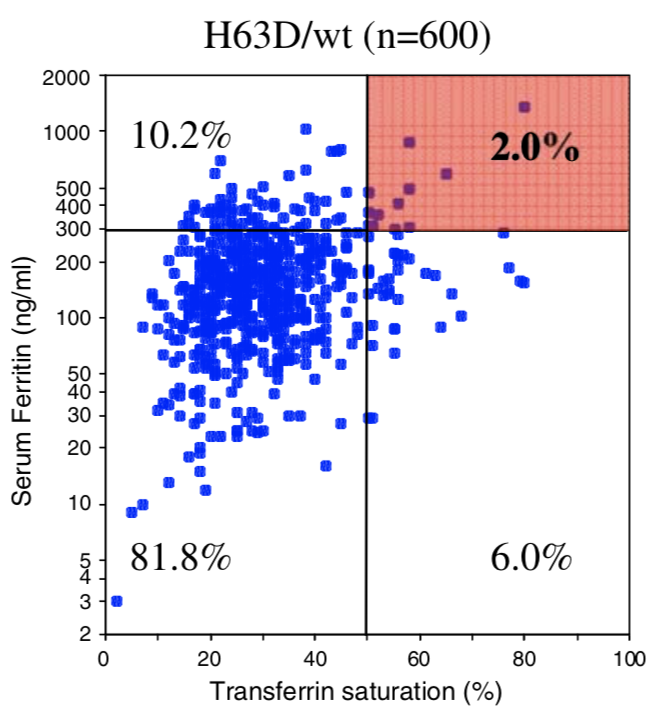 | 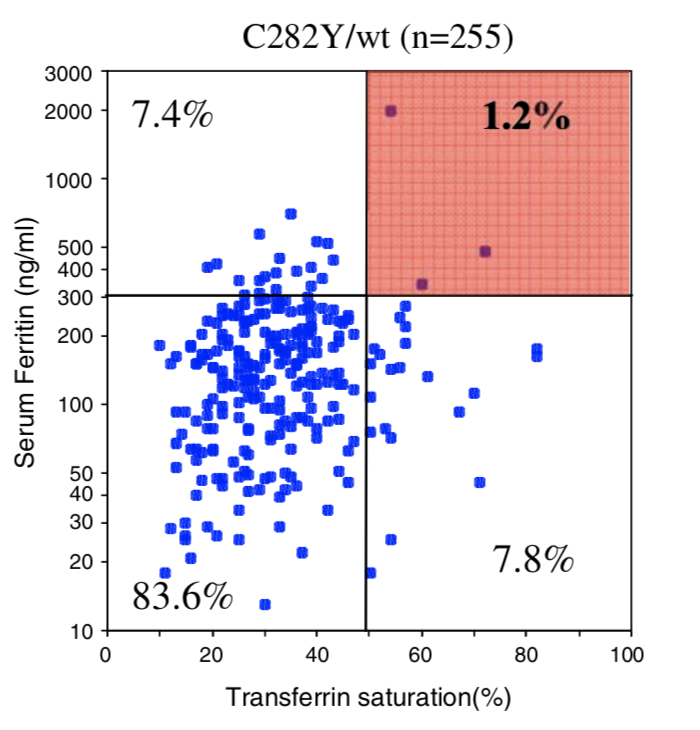 |
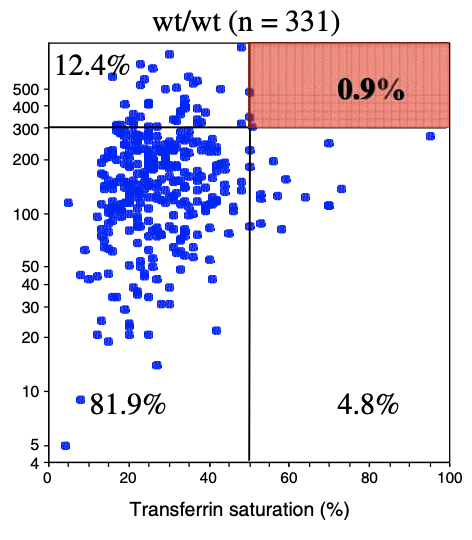 |
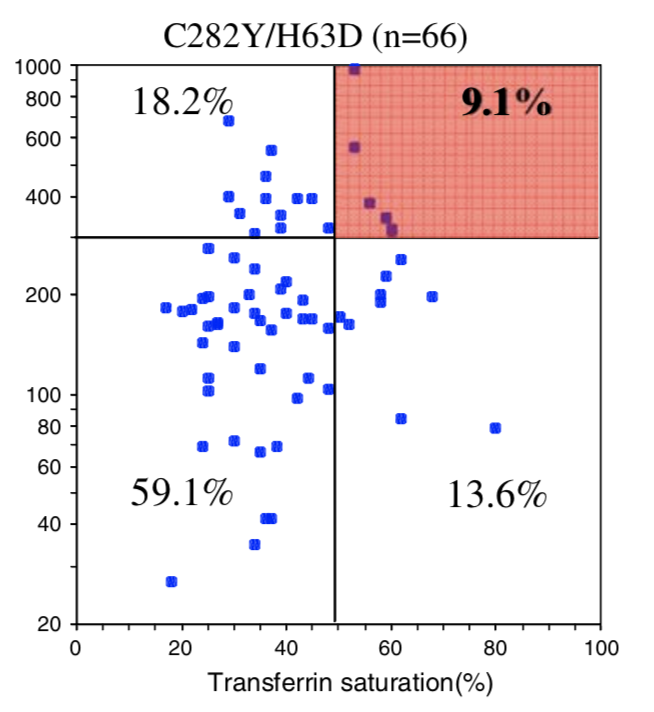
| Biological Penetrance | 76.5% | 9.1% | 5.4% | 2.0% | 1.2% | 0.9% |
| Age range for symptoms | 16-100 years | 34-100 years | 41-100 years | 41-100 years | 33-100 years | uncertain |
You can see from the above table that there are massive age range for all the HFE Gene mutations and their combinatons but for the lower penetrance ones the age range is slighly less. The reason for this is that the homozygous C282Y mutations causes the strongest iron loading, whereas the carrier (single mutation) examples have much slower loading rates. But this still does not explain why their is such a wide age at symptoms range for all cases. And the reason for this is there is something else going on. It could be 1 of 2 reasons or both of these:
- Either a lifestyle thing - different people eat different iron containing food or regularly loose blood for example via blood donation
- Or, another mutation is having just as large effect as the HFE gene.
The reality it IS going to be both but it appears based on our data that in reality it is for most people mostly the effect of other mutations
Now let's look at what's going on here.
![]()
The diagram shows a simplified view of what is happening with iron in the body. There are 3 layers involved, the stomach wall, the blood and then the organs. Classic Iron overload is mostly concerned with too much iron in the organs and it accumulatives over time. But serum iron overload (SIO) also exists as a lesser complication with different symptoms. SIO needs to happen before organ iron overload (OIO) can occur. Whereas SIO is dependent on a defect in Hepicidin production for Hemochromatosis Type1, OIO is dependent on Transferrin production to carry the iron into the organs and mutations of the Transferrin (TF) change the rate at which this happens. This classic organ iron overload is dependent on 2 genes and defects in both genes either increases or decreases the rate at which the iron overload accumulate. It is therefore the mutations of both HFE and TF genes which determines what age we will overload. Throughout life the iron in our organs accumulates and when it gets to a point where it becomes too much then the damage to the organs starts to occur and we experience the autoimmune symptoms of iron overload.
The important thing to realise is we measure the ferritin and transferrin saturation in the blood to determine if we have iron overload but this is an approximation to measuring the iron stored in the organs. As it is, the excess iron in the organs which causes the majority of the medical issues. The HFE gene mutations controls the rate at which the iron flows from the stomach wall into the blood-when a person has one of the Hemochromatosis mutations the bodies is less able to make a protein called Hepcidin. In healthy people Hepicin controls the rate of flow of iron into the blood stream - if the body has enough iron the body can request that no more iron comes in - in Hemochromatosis this request does not work as well and the iron continues to flow in.
The above is a simplification and really only describes the way Hemochromatosis Type 1 occurs. Other less common conditions can complicate everything much more and we'll discuss these in a future article.
![]()
To further complicate matters if we have the mutations to cause Hemochromatosis and we also have Gut issues such as Gluten Intolerance or even an ulcer, there is a more direct means of iron and other poisons getting into the blood. This means those with the mutations will experience unimpeded iron flow into the blood. So it then just takes a TF mutation which increases Transferrin to then cause more iron to flow into the organs. The worst thing a person can do with Gut issues is to eat fortified breakfast cereal which contains pure iron already which can just cross the gut barrier with no problems. These fortified breakfast cereals can also damage the gut biome because the presence of iron can change the gut biome balance promoting the growth of potentially pathogenic enterobacteria species at the expense of protective lactobacilli and bifidobacteria species
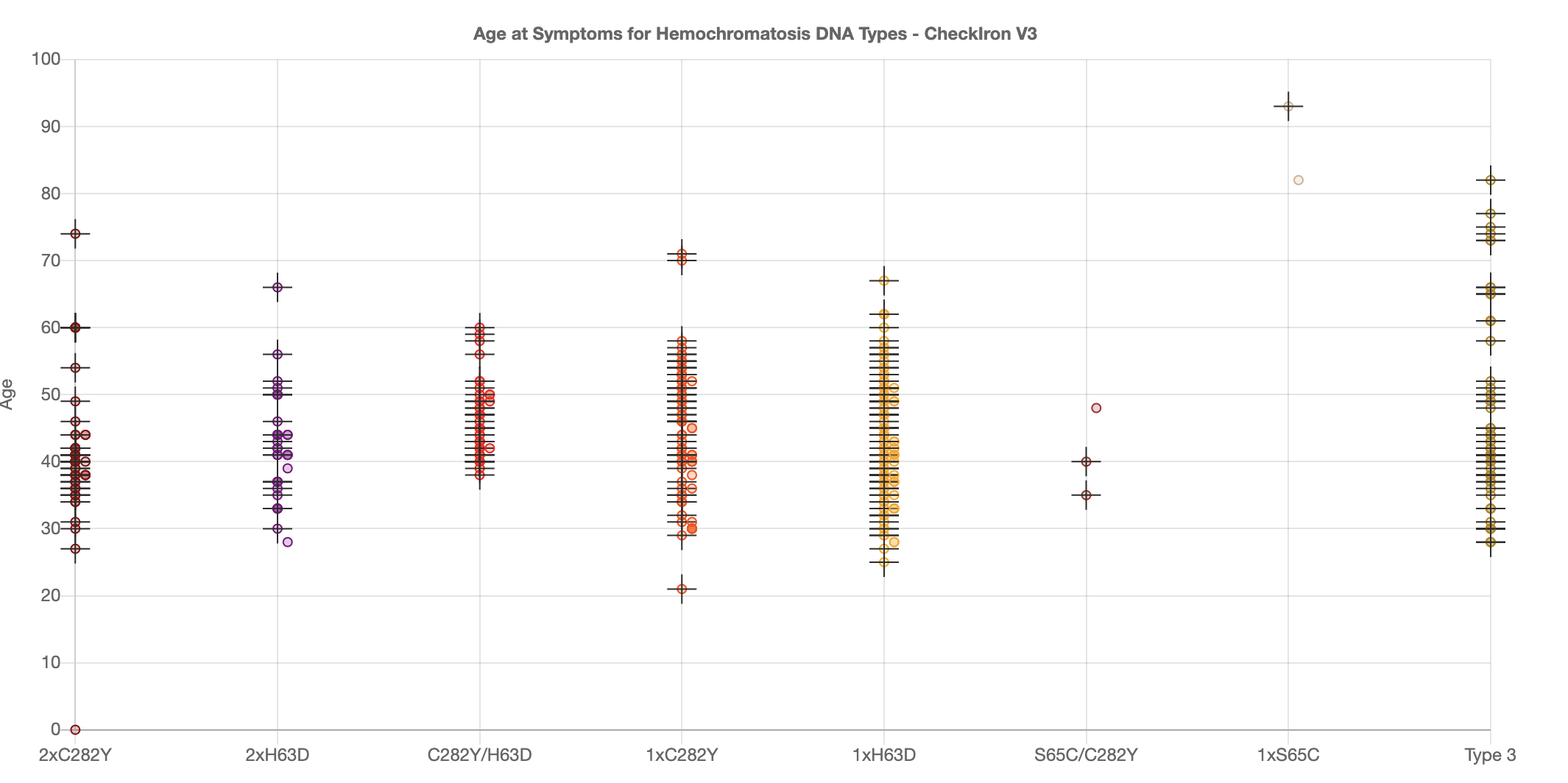
CheckIron is now getting more and more people who upload their data and for those that have been ill, they tell us the age when they got symptoms. This
is very useful for it allows us to perform data analysis on the data to determine what mutations are causing their symptoms. The graph below shows for the different HFE mutations the variation
in age of symptoms is wide for all types and imediately implies there are other factors causing this wide variation. This could be lifestyle effects such as diet but we have found we do get some
correllation with other iron metabolism gene mutations and the gene mutation risks of other auto-immune diseases.
Nearly everyone will say Hemochromatosis is a monogenic diseases which means its dependent on the single HFE gene. However, scientifically this has never been true:
So we do conclude Hemochromatosis is indeed a polygenic disease and as such carriers of one of the genes involved can suffer hemochromatosis.
There is a very good scientific paper explaining the Current understanding of iron homeostasis from 2017 which explains this process very well
Diagnosis
Of course, if you take part in prevention and are successful you do not need to get a diagnosis. So in the ideal situation no-one should be diagnosed ever, let alone suffer from symptoms. However, very few people believe prevention is possible (except those that understand what checkiron has achieved ) so Diagnosis is still very necessary especially as 90% of Hemochromatosis suffers are never diagnosed until they die from it - often found at the autopsy.
The best document from BSH (British Society of Haemotology) about diagnosis is at Diagnosis and therapy of genetic haemochromatosis (review and 2017 update) This BSH web pages reference the original PDF document. Do not bother with other documents from other sources such as Haemochromatosis UK charity which has very poor, incorrect and inconsistent information. However, even this document does not talk about using Genetics to predict risks from Iron Overload as these discoveries are too recent for them to be both accepted and included in this document- these BSH Guidelines are still the best official documents around, so don't read others who claim to be better.
It's important to understand the 4 stages of HH diagnosis:
- Prevention - this is treatment because of the existence of genetic risks before any symptoms are observed, including before raised blood iron panel levels. Nearly everyone says this is impossible because the common medical genetic tests cannot predict when or even if someone will get sick from there particular gene configuration. CheckIron is the first to claim this is possible using commercial DNA tests and not the medical tests which always test for too few genes.
- Biological penetrance diagnosis - this is treatment because of existence of raised Serum Ferritin and raised Transferrin Saturation. For Homozygous C282Y (the strongest form) the biological penetrance is 80%, meaning 80% will suffer raised iron levels corresponding to Ferritin>300 and Transferrin Saturation % being >50% before they die and 100% loading iron faster than someone without the mutations. The 20% difference is that some people die early from something else and some load more slowly due to other genetic mutations.
- Organ Iron Overload. Detection of iron levels in organs such as the liver. This used to be via liver biospy but is often now done via MRI Ferriscan to measure the amount of iron in the liver. The maximum amount of iron is normally 1.8mg/g with iron overload people having more than this and often many times this value
- Clinical Penetrance. If Biological penetrance has not been spotted and more untreated years have passed, then we enter Clinical Penetrance. This is more than just organ overload it's where the liver and other organs such as the heart and pancreas, as well as the joints are damaged by the high levels of iron. The individual will also feel ill in this period but not know the reason why. It used to be that only this point when the first detection was performed and many of the dialogue on some of the Facebook Groups seems to assume this is still the case; you often see people saying the penetrance of Homozygous C282Y is 10% for women and 20% for men. This assumes detection is when damage has already occured. Since nowadays this point should becoming less frequent because of success of Biological Penetrance being detected you'd think its no longer important. However, the problem is 90% of sufferers still do not know they have the condition and organ damage is all too frequent.
At any stage treatment can start and help stop the transition to the next stage but be aware the later in this list that diagnosis occurs the worse the outcome. In the case of the liver, light damage can be repaired by regeneration but for the heart, pancreas and joints there is currently no repair option (although anti-aging technology will make that possible in 10 to 20 years)
The other inflammation problem for Doctors
It's a fact that any inflammation not due to HH will cause a spike in Ferritin blood levels. So when a doctor sees high ferritin he does not immediately know whether or not HH is the cause or even a partially contributing cause. If the Transferrin Saturation percentage is >50% for men and >45% for women then that indicates is more likely HH, especially if the Ferritin level is >1000. There is also a blood inflammation measure called CRP which can indicate just inflammation and liver enzyme details could help predict liver damage - but the liver is always late in showing damage - when damage is indicated its often after more significant damage has been done. So, for the doctor this is a major issue and if a doctor sees evidence of inflammation even though genetics may suggest high risk of Hemochromatosis, many will choose to ignore Hemochromatosis and and therefore refuse Phlebotomies. Some doctors also do not believe carriers can get iron overload and the problem is that carriers also do not usually get as high Ferritin levels as Homozygous C282Y people, so this confusion is exacerbated further. Some doctors refuse to treat carriers with iron overload. The problem is we (at Checkiron) believe that the 1.2%-2% of carriers who really do suffer iron overload do so because inflammation from non HH sources IS involved in addition to excess iron from mutations causing hepcidin deficiencies - this is a digenic effect (involving multiple gene defects not just a single HFE gene defect). This belief is not accepted by the doctors but IS considered a real effect by the scientists involved in investigating the iron metabolism. This issue is made worse because some doctors do not accept even non C282Y mutations from H63D and S65C as being contribuary to iron overload- this includes mutations involving 2 genes such as 2xH63D and compound C282Y/H63D which usually result in weaker but still real load modifying speeds. The thing doctors need to realise is that if they think the evidence in the blood work in not sufficient proof (or border line) they still should check for liver iron levels using MRI Ferriscan as in many instances they will discover unequivocal proof of organ iron overload.
Treatment and Maintenance
For most people, treatment for Hereditory Hemochromatosis (HH) is simple and effective; it’s a form of regular blood donation known as "Phlebotomy" in most countries and “venesection” in the UK. Initially, your doctor will ask you to attend hospital or a clinic weekly or fortnightly to have up to 1 unit (450 ml) of blood drawn. This has the effect of stimulating the body into producing more blood, which draws excess iron out of the organs and soft tissues. Then – a week or two later - another unit of blood is drawn, and the process repeats. You’ll need to have a venesection regularly until your serum ferritin (SF) is between 20-50 μg/l and your transferrin saturation (TSAT%) is below 50% for men and 45% for women. Depending upon your iron levels at initial diagnosis, it may take several months to several years of phlebotomy/venesection to reduce your iron levels to normal. Phlebotomy/Venesection isn't always an option for people (for example, if venous access is consistently troublesome); for a small number, alternative therapies including chelation may be used instead (or interchangeably). These approaches use drugs administered orally or by injection which bind to excess iron to enable it to be passed out of the body. Different medically available drugs are available, these include Deferoxamine, Deferasirox and Deferiprone. A workable alternative is IP6 supplement which you'll find on Amazon - this is made from the husks of rice and you need to be careful as to the source of the material as the rice it is made from could have large levels of Arsenic in it. Chelation has some downsides as they Chelate all di-valent minerals from the body - not just iron, so when you reduce iron you also are reducing copper, zinc and magnesium - because this, chelation should not be used as a long term option
One aspect of Phlebotomies is that sometimes people find that during the de-ironing they actually feel worse and get more inflammation with the TSAT% rising whilst the Ferritin level falls. This is quite normal and some say it is due to doing the Phlebotomies too often/quickly. This is certainly due to an in-balance and it affects slow loaders the most. If you were a slow loader (getting symptoms later in life) you will be a slow unloader too and it will be easier to throw your system out of balance. It might help to do the Phlebs less often but often this is not practical, so this is often something you have to live with during the de-ironing. Also when you reach maintenance your system can also be out of balance and again ferritin can end up <50 but the TSAT% >50% - this is commmon and many people worry something is wrong when actually, it is to be expected. There is also a lot of mis-information spread about this state which is totally incorrect and non-scientific. One of the US based HH sites mentions something call Iron Avidity and some members of FB Groups try to use this concept to describe what happening. But the concept of Iron Avidity has been made up by someone who did not understand what is really going on here - their description is the opposite of what is actually happening. In this case the iron is being pulled out of the liver and actually becoming free elemental iron in the blood stream. This increases Serum Iron and increases inflammation, making you feel unwell (it's observed as high TSAT%), but its due to de-ironing and not the body trying to absorb more iron. In most cases when this happens in Maintenance, we find that after a few Maintenance cycles this state improves and eventually the TSAT% reduces to around 30-35%. When Ferritin is <50 and TSAT% is 30-35% you are now in balance and if you are also a slow loader you may have the capability of controlling your loading use diet rather than relying on maintenance Phlebs. Fast loader will probably always need to use Phlebs to control it.
Some people have this low ferritin and high TSAT% state for years and it does not go away. This is actually something to be concerned about and you should try to discover why this is happening by discussing with your doctor. There is a mechanism using the ceroluplasmin protein which converts pure iron to ferritin (ferritin is a safe form of iron) - it is used by the immune system to control the inflammatory effect of pure iron and conversely the immune system can increase the pure iron to increase inflammation using macrophages to deliver the iron. So iron is inherently a soldier used by the immune system to increase and decrease iron. If you suffer from an autoimmune disease this may be a factor in this happening. It is particularly important that the individual is not Vitamin D deficient and if this is found to be the case they should ask their doctor if they need to take vitamin D3 supplement. I've seen one strongly opinionated (and often wrong)individual state that this state is iron deficient anaemia - I don't believe that would be commonly the case so long as the ferritin were above 20- in any case anaemia can be spotted by seeing out of range low HGB levels. What is more likely is that there is an issue with the ceroluplasmin production, this could be, either due to a gene defect of the CP gene (in a disease called Aceruloplasminemia) in the making of this protein or a copper deficiency. Copper is needed to make ceroluplasmin and if you are not getting enough bioavailable copper in your diet and/or you are using up copper quickly because you are making ceroluplasmin then you could get into this state. Beaware though that in large amount copper is a poison so do not take bioavailable copper without consulting your doctor first and then following their instruction precisely.
Diet
For all people with or without Hemochromatosis, a good healthy diet is essential. With the western diet containing too many carbohydrates and especially too much sugar we would recommend for all people that they consider a low carb/high fat diet such as Keto. This is particularly valid if you are already suffering from Diabetes Type 2 or have a fatty liver. A limit of processed foods is also a good idea too.
For those diagnosed with Hemochromatosis you often read the following:
- that you need to avoid iron and vitamin 'c' supplements
- if drink fruit juice do so between meals not during a meal
- don't consume fortified breakfast cereals which contain unnatural pure iron additives which when combined with gluten intolerance could cause considerable harm as the unprocesses iron can go straight through the stomach wall into the blood stream and wreak havoc.
- avoid raw shell fish because they could contain a bacteria which multiplies in the presence of high iron and could make you very ill.
- limit alcohol consumption especially if you believe your liver has been damaged. Also be aware that alcohol increases iron levels in the liver and can cause fatty liver too.
Many people in the FB Groups will say once you've obeyed these rules, then it does not matter what you eat including steak because you just get more Phlebotomies if your iron levels increase as a result. However, its our belief this is just a dumbing down of the truth so much it is no longer true for most people. For us this is equivalent to saying you can jump off a sky scraper because there is a safety net at the bottom - the problem is you can still get hurt in those circumstances so why would you do it. The truth is the effectiveness of using diet to control the rate at which you load iron depends on you genetic measurement of your loading speed which checkiron gives you an estimate of. If you're a fast loader and you originally got ill in your 20s (or even earlier), then using diet to control it will be largely ineffective. In this case the genetics faults are so severe what you eat will only have a minor effect and you will need to rely on Phlebotomies - so in this case and only in this case are those statments that it does not matter valid. The truth is most sufferers are not in this position, most people are medium speed loaders or slow loaders and in these circumstances diet does indeed have an effect and we'd recommend you don't rely in the safety net of Phlebotomies, if you find diet does help (or at least consume less iron so that you do not so many Phlebotomies).
Worried? Don't Panic
If the DNA analysis has told you, you are at risk of Iron Overload but you are worried because you don't understand what this means, the important thing is not to panic. If you have this condition it is fully treatable so long as not too much damage has been done. If you used CheckIron, we will also have given you an "Age at Symptoms" and for some people this may be worrying, particularly if the age is in the past and you don't yet have symptoms. This age is very much an estimate and it is not yet very accurate -so you don't need to worry. If you are at risk or even if you have any concerns consult your doctor and ask for an iron blood panel test which tests Ferritin and Transferrin Saturation. Note that some doctors will only do the Ferritin test to start with. Also if you are a carrier for Hemochromatosis some doctors will not believe you have any risks although see our prevention article to see what the official risks really are. In our view (although not yet accepted by the experts), we see from the data that carriers have between 1 and 2% chance of overloading iron but this these risks are significantly increased if you have 2 or more mutations of the TF gene which speed up loading. Clearly there are other conditions which speed up loading so you definitely should consult a doctor to get an expert opinion on you personal medical condition - note everyone is different in reality.
If you have the risk mutations of the HFE gene, your doctor should perform an iron panel blood test. Iron levels acuumulate over time, so even if you have a negative result, your doctor should schedule at least yearly tests. If the doctor sees at large Ferritin level (close to or above 1000) plus a Transferrin saturation percent above 45% for a woman or 50% for a man then this would indicate a higher risk of iron overload. In some case doctors consider this enough for a diagnosis but others consider a measurement of the amount of iron in the liver to be needed for confirmation. A form of magnetic resonance imaging (MRI) scan called FerriScan or LiverMultiScan (these are brand names) is now increasingly in use as a way of directly measuring liver iron concentration. MRI is usually preferred to biopsy as it is cheaper, non-invasive, quicker and more accurate. However in some cases a biopsy might still be necessary; a small sample of the liver is removed using a biopsy needle, which is checked to see whether tissue damage such as cirrhosis is present. Liver transient elastography or Fibroscan (a brand name) is similar to an ultrasound scan and is widely used as a way of checking for fibrosis and more severe forms of liver damage such as cirrhosis.
If you have the gene mutations you should consider there are risks for your children, parents, sublings, cousins and aunts and uncles. You should inform your relatives and suggest they also have their DNA checked. This can be done by a doctor or using consumer DNA analysis company and then CheckIron. These 2 types are equally accurate but since the commercial tests, test for many more mutations they are very much better (this latter statement might be considered contraversial by some people).
Once you have a diagnosis then treatment is arranged. The most efficient way to get rid of iron from the body is to do a regular Phlebotomy (called Venesection in the UK) which means taking 1 pint of blood every 1-2 weeks until the ferritin level is decreased. This process will take months or even more than 1 year in some cases. Once the ferritin level is down to 50 then you are deemed to be in maintenance. At this level the Phlebotomies need only doing every 3 months or in some cases 6 months. When in maintenance you are no longer suffering from iron overload and for many countries blood donation is also allowed which can be a useful alternative to Phlebotomies. Note that even when the ferritin level has decreased the Transferrin Saturation is likely to stay high to begin with, but this too will eventually fall. The case of low ferritin and high Transferrin Saturation is sometimes called Iron Avidity (there seem to be some myths put out around about this state, Ignore these stories, they are usually meaningless.)
Inflammation
The Cause and Effect Tree involving Iron(Fe) and Inflammation
Cause and Effect within the Human Body is more often than not confused and misinterpreted by Doctors. It IS complicated because there is often a chain of causes and effects and additionally there can be a feedback loop where the effect links back to the cause.
These 2 complications are particular true for Inflammation. We show a typical Cause and Effect tree in the picture below for Inflammation and furthermore we spell out the Role of pure Iron in the inflammation story which is nearly always ignored as though its not highly signifcant as it really is.
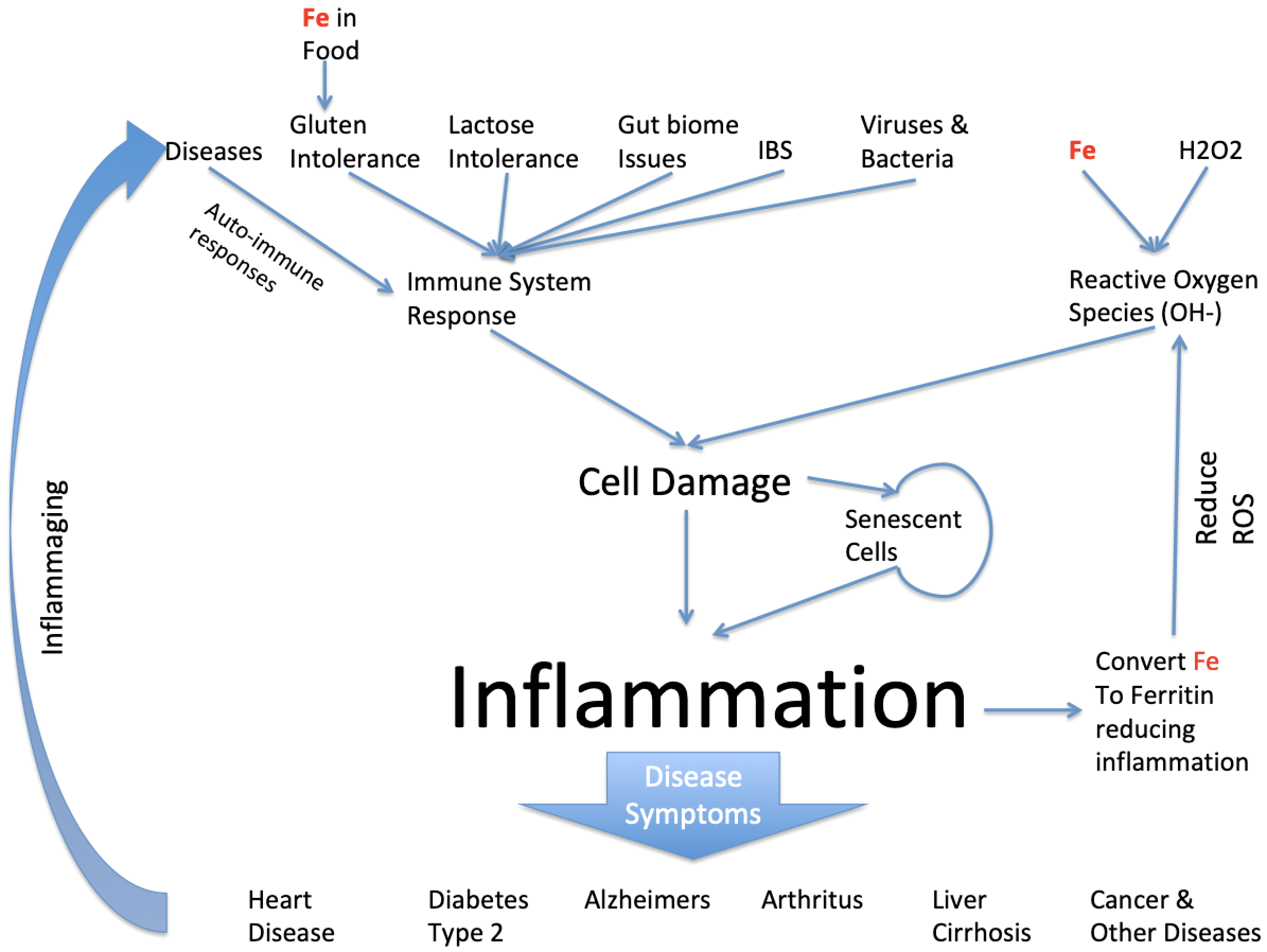
Clearly inflammation can be caused by a large number of things but we're particularly interested in the role iron takes in this and it does so in a number of ways. First iron enters the body through food eaten and usually in a biochemical form. However, when iron is added to foods for alleged nutritional reasons the iron is more often than not added as pure iron. Pure iron is highly toxic in conjunction with Gluten Intolerance it can enter blood stream directly and cause havoc by inducing inflammation from creation of Reactve Oxygen Species (ROS). The pure iron reacts with natural small amounts of natural Hydrogen Peroxide in the body resulting in Hydroxyl ions which are highly damaging to cells it comes across and cause inflammation. The body always has some naturally pure iron because the immune system of a healthy person can control how much there is. But if the person has Hemochromatosis this is not the case.
Meanwhile there are many other factors involved in the creation of inflammation. Its main existence is due to the immune system attacking foreign invaders such as Viruses and Bacteria. The side effect of it is that it can also attack close by healthy tissue. The immune system will also attack milk products if the person cannot process lactose and this also causes inflammation. Once a cell is damaged it can effectively stop working but its left in a senescent state. Senescent cells can infect close by cells making them senescent too and causing further inflammation. There are mechanisms to remove senescent cells but I'll address that in a separate article.
Dependent on where in the body the inflammation occurs results in the disease we observe, so in the heart its called heart diseases, in the brain its called Alzheimers or Parkinsons and as a result of being in the pancreas with observe diabetes because the person has insulin resistance and cannot control their blood sugar levels.
And my point was that iron is very significant in this story both as either excess iron because its been build up in the body because of old age and for the 1.25% of the population with the most common genetic disease of Hemochromatosis its highly significant as it can be a significant contributor to all or some of these inflammatory diseases. Another point is that the other root causes such as Diabetes, Gluten and Lactose intolerance are also genetic risks.
Since all these diseases are mostly age dependent and which ones we suffer from are dependent on our genes, I want to ask the question can we predict, given knowledge of our DNA, what age you will suffer from one or some of these diseases. Clearly lifestyle (ie what we eat) comes into this too but assuming most people have similar lifestyles can we infer from genes what age someone will start suffering from these Inflammatory diseases. Now I run a website (called Checkiron.com) which helps people that suffer from Hemochromatosis. Its been running 12 months and I’ve been collecting their DNA data and asking them when they got symptoms- we then use Machine Learning techniques to learn and then infer from a new DNA dataset when someone will get symptoms. To start with I was just looking at the genes involved in the Hemochromatosis disease and this worked for the extreme cases when people got inflammatory diseases in their 20s but it worked less well for the weaker forms of Hemochromatosis and we discovered from the data it was things like Diabetes Type 2 disease that were having a significant affect on the “age at symptoms”. Simply because all these symptoms of inflammatory diseases are indistinguishable for the patient and the doctor treating the patient. The result is that currently for people with the Hemochromatosis mutations we can predict to +-12 years when someone will get bad symptoms. Furthermore since Hemochromatosis is entirely treatable, if caught early enough, we can say at what age, this preventative treatment should be taken. This approach could save 100s thousands of lives each year of Americans suffering from HH and not knowing it. Furthermore since this disease runs in families then those that detect the issue could suggest to other family members they should check.
Myths
10 Myths of Hemochromatosis
Myth#1 It does not matter what you eat.
This is a case of people being told something they want to hear. But since what you eat defines your health to a great extent this is far from being correct for most people. However, if you are a fast loader (ie you got sick in your 20s), you are heavily dependent on Phlebotomies to control the iron levels. In this case there is a valid argument that since you are doing regular iron removal it matters less what happens in between. However, with unfettered iron consumption you may be putting the body under more strain than is good for it and I'd still argue its better not to do this.
For slower loaders it's clearly obvious that what you eat does matter and eating less iron can in many cases prevent the need for any Phlebotomies. Surely this is clear cut, you should eat less red meat, no liver or offel and avoid vitamin C when eating - no orange juice with meals. Also alcohol needs to be treated with great care as this does increase iron intake in the liver and can increase damage.
Myth#2 Hemochromatosis is due to mutations of a single Gene called HFE gene.
Most genetic tests, test just 2 mutations of the HFE gene and then people wonder why there can be a age range of more than 60 years between different people with the same mutations getting ill. It's clear the reason for this age range is due other genes changing the iron loading rate - the scientists have known this for years and the fact is the Transferrin Gene and two of the BMP genes change the loading rate. Doctors seem to ignore these published scientific findings and as a result make statements that their Hemochromatosis genetic tests cannot be used to predict whether someone will get ill or not when by looking at more genes as does CheckIron this can be predicted relatively accurately.
Myth#3 You need two mutations of the HFE gene to get Hemochromatosis
Hemochromatosis is supposed to be a recessive condition requiring 2 identical mutations to cause the Iron Overload problem. However, the scientists have measured the probabilities for all the combinations of possible mutations and the chance of getting Iron Overload is non-zero for all the combinations. Carriers with Hemochromatosis are between 1-2% chance but this is a finite level and depends on other genes and other risks of inflammatory diseases. This is disagreement between doctors in this are resulting in 3 groups 1) Doctors believe on Homozygous C282Y suffer and only men 2) Doctors believe any 2 mutations are needed but with reduced risk for the individual 3) A small group of doctors believe carriers and 2 mutation people can suffer. The fact doctors don't agree shows the mess we are in. Even the UK Haemochromatosis Charity do not believe carriers can load due to the HFE gene mutation.
Myth#4 Young suffering people have Juvenile Hemochromatosis
When a late teen or 20 something person gets Iron Overload people assume its Juvenile Hemochromatosis. The the chance of this is about 1 in 2million but usually in these cases its a strong form of Homozygous C282Y more often than not. ie fast loading homozygous C282Y.
Myth#5 Vitamin D deficiency is good for Hemochromatosis sufferers.
This myth is completely false and yet it has spread on Facebook Groups and even appears in one of the Hemochromatosis books. The reason it's stated is that scientists have done studies on the effect of Hepcidin production when someone has chronic kidney disease - they discovered that Hepcidin decreased for these people when they took Vitamin D supplements. So this was not people with Hemochromatosis who have a genetic fault. Vitamin D deficiency is also a fault - Vitamin D is an essential hormone that regulated the immune system - being deficient in it is also a fault. 2 faults do not make a right - its insane to make the assumption this would affect Hemochromatosis people in this case. People should not take this one seriously at all.
Myth#6 The medical DNA tests are better than the commercial DNA tests
There are two aspects to DNA tests 1) Accuracy 2) Coverage. The accuracy of all tests is very high and my guess is the automation used by the commercial suppliers perhaps reduces the possibility for human error considerably. It's really the coverage of the test (this is the number of genes and mutations looked at) which is the major difference between the medical tests and commercial tests. The medical tests usually look at just 2 mutations of the single HFE gene whereas the commercial tests are looking at 700,000 mutations of ~ 20,000 genes. Clearly the 700,000 is more than is needed for Hemochromatosis but we believe that ~1,000 mutations provide useful information to the contributors to Hemochromatosis symptoms as well as the speed at which the loading occurs. There's really no comparison here, the commercial tests are 1,000s percent better and more informative.
Myth#7 There are 5 different genes that can cause Hereditory Hemochromatosis but only Type1 (HFE gene) is not rare.
This is wrong. Hemochromatosis Type 3 (the TFR2 gene mutations) is actually nearly as common as Type 1 (the HFE gene mutations) and is not rare. Also someone can commonly have a mixture of Type 1 and Type 3 at the same time. This makes a further mockery of the medical genetic tests which only test the HFE gene. Types 2, 4 and 5 are very rare though.
Myth#8 The "penetrance" of Hemochromatosis is 10% for women and 20% for men.
In exact detail this myth is true but its still a myth because it's incorrectly used to describe why small numbers of people with risk mutations get sick. This word "penetrance" should say "clinical penetrance" - this means the percentage of people who get so sick that severe liver damage or heart disease occurs and probably die early as a result. This is the state of the disease no-one should get to as you want to detect the risks before any organ damage. For this reason more sensible doctors have invented a term called "biological penetrance" - this occurs when the blood panel tests show iron overload symptoms - at this stage the patient might well have arthritis and/or heart palpitations but easily treatment should result in the person getting better and never reaching "clinical penetrance". So measuring and using clinical penetrance is pointless since over time as doctors get better at recognising HH the clinical penetrance might actually reduce to zero (hopefully). So it is a myth that small people suffer iron overload for example homozygous C282Y men have a biological penetrance of 80%. Furthermore it is even more correct to say 100% of homozygous C282Y men will start to load iron but 20% may die of something else before iron overload is reached.
Myth#9 There is such a thing called "Iron Avidity"
This term was invented by 3 doctors in 2004 and picked up by the iron disorders institute and promoted by them as a real condition - its also often mentioned on Facebook groups as though it really exists. However, no other Hemochromatosis institution recognises it. It describes the case where a person has low ferritin and high transferrin saturation - this condition IS real and can have multiple causes. The problem with calling is "Iron Avidity" is that the description is the body is trying to acquire the iron in the organs - the problem with this description is that it does not match any real science and is often the complete opposite of what is really happening. The real condition of low ferritin and high transferrin saturation can actually occur and is usually a result of some in-balance. For example, it is often seen at the end of de-ironing when the patient is about to or has achieved maintenance - at this point the ferritin has reached maintenance level but the liver is still being drained of iron resulting in serum iron remaining high which causes the transferrin saturation to be high. This in-balance can also be seen for 2 other reasons: 1) the patient has copper deficiency resulting in the deficiency in the enzyme ceruloplasmin which normally converts serum iron to ferritin 2) the patient has Vitamin D deficiency resulting in the immune system being out of balance and therefore the iron levels out of balance.
Myth#10 Iron fortified foods have no effect as the iron levels are not significant
Typically a bowl of fortified cereal has 4-8 mg of pure iron in it. The reason for adding pure iron is to help the 10% of the population who suffer from Iron Deficient Anaemia (IDA). The reason why they use pure iron rather than an iron salt as used in iron supplements is because the dose in food is undefined there is a concern of iron over-dose particularly for children. The theory is iron salts absorb more quickly and there have been cases of poisoning of young children from too much iron salt supplements. The idea is that pure iron needs to be converted to a salt using stomach acid before it can be absorbed- the hope is it is then absorbed more slowly causing less poisoning. In a healthy gut this may be correct, but many people suffer from leaky gut, or, IBS or, stomach ulcers and in these cases this theory is very very wrong. If you have gut problems then pure iron becomes deadly and will poison someone faster with dire consequences if these cereals are eaten regularly - this problem is worst for Hemochromatosis people but even for non Hemochromatosis suffers it can also be a problem as the natural Hepcidin absorption control is being circumvented. In Denmark this problem has been recognised and iron being added to food is banned. Although other countries have tried to do this no others have yet to succeed.

FAQ
FAQs
None of the below should be considered medical advice - we are describing the questions people ask about Hemochromatosis. Always consult a qualified medical professional.
- Official Recommended Procedures is to do Iron Panel Tests before Genetic tests. Why are you saying something different?. These procedures were created at a time when it was not known that DNA could fully predict the "age at symptoms". Since this is now known those procedures are now invalid.
- Only 10-20% of people with the HFE mutation get Hemochromatosis. So what is the point in doing a DNA test?. This 10-20% number is for clinical penetrance which happens when the organs are damaged. Now we know someone has HH when they reach Biological Penetrance clinical penetrance is now a meaningless condition since more and more people are being treated at Biological Penetrance.
- It does not matter what I eat for iron and HH. Do you agree? This is a simplification which has been blown out proportion by being repeated too many times by people who don't understand what's is purpose is. If you as a HH sufferer with iron overload are under-going phlebotomies then it does not matter what you eat within reason because your condition is being treated by the much stronger effect of Phlebotomy. However, before Biological Penetrance is reached or after maintenance is attained it is better for the body NOT to be subject to the inflammatory effects of too much iron.
Sample Data
You may be interested in seeing example data for different people with different mutations. Why do different people with the same HFE mutations overload any where between age 20 and age 70? The answer is the other mutations are affecting the iron loading rate. See deifferent people with different loading rates affects their age at symptoms figures. These datasets are based on real people but have been altered slightly so there is no connection to a particular real person.
The examples are as follows:
- Homozygous C282Y with fast loading
- Homozygous C282Y with slow loading
- Carrier H63D with fast loading
- Compound C282Y/H63D fast loading
- Compound C282Y/H63D slow loading
Future of Hemochromatosis
Hemochromatosis prevention, diagnosis, and treatment have not progressed in any meaningful way for the past 20 years. Maybe MRI ferriscan has been an improvement instead of liver biopsy, but there has been a lack of reliance of DNA testing. This is very disappointing because in that period cost effective DNA tests have been developed for the consumer which are many times better than the medical tests and the scientists have discovered much more about the disease too and yet the approach for diagnosis have remained as blood tests and treatment has been unchanged for the last 3000 years. Meanwhile prevention is not considered possible and DNA is only used AFTER a blood test has been identified. It's true medical procedures talk about testing relatives using DNA, but I personally have not seen this put into practise.
One positive achievement of the past few years is the acceptance by most doctors that biological penetrance is used rather than clinical penetrance to work out the number of people affected (although one of the UK's Hemochromatosis charities remains in the past in this matter). Most doctors accept that the biological penetrance is 80% for C282Y - this means if you have two C282Y mutations then you have an 80% chance of suffering iron overload. This should be compared with how it used to be where clinical penetrance numbers like 10% to women and 20% for men used to be used and note one of the UK charities is so out of date they still use these figures. What they don't realise is that the 20% who do not suffer biological penetrance are still loading iron just at a slower rate such that the iron overload cutoff is not reached before they die. The problem remains though that for other mutation combinations many doctors do not believe the risks are significant even though penetrance for compound H63D/C282Y is 9.1%. What is even worse is the real number that should be recognised is (penetrance * prevalance) and even though the penetrance of carriers can be between 1.2% and 2% the prevalance can be as high as 20% in some countries. The result is that because on average 1 in 12 people are carriers the number of carrier sufferers is 44% of all sufferers - this is why its quite common to see carriers commenting on the FB Groups even though for any one carrier the chance of suffering can be as little as 1.2%.
In the medical procedures DNA tests are currently used to confirm a blood iron panel test measurement and suggested for relatives only of Homozygous C282Y. Other forms such as compound H63D/C282Y and Homozygous H63D with lower chance are also down played by many doctors as not really being Hemochromatosis and this seems to be a low percentage chance is treated as though it will not happen.
This all has to change in the next 20 years and actually I'm sure it will. There is also another revolution in genetics on the way. One of the problems with the commercial DNA tests is that they are looking at 2% of the human genome and difference companies are looking at slightly different 2% with some overlap (this is actually not as bad as it first seem because the 2% looked at is the most important 2%). Although this is thousands of times better than the medical tests which look usually at just 2 mutations of the HFE gene, it's still very unsatisfactory and gives incomplete comparisons between people with partial support for the diseases being examined. The solution is cost effective whole genome sequencing (WGS), this now seems to be coming available as prices of $300 now seem possible, although all these offers suggest a subscription in addition which provides updating reports. In the next few years the costs will continue to fall and we expect to reach the $100+ range.
Other future improvements are that we do believe everyone in developed countries will eventually be getting WGS tests and true preventative medicine will be practised for many diseases and in particular for Hemochromatosis it will become the accepted approach whereas today there is no acceptance of that whatsoever.
Additionally as the scientists discover all the iron metabolism pathways we will start to see m-RNA treatments such that regulation of Hepicidin via a virus delivery of m-RNA will be able to regulate iron flow whilst still having the faulty gene present. These are exciting times for medicine as the importance of Genetics and Epigenetics being used for prevention and repair begin to be used causing a revolution in medicine.